[For a refresher on how this effort fits into the bigger
picture of chemical assessments, you can review my infographic.]
So far, the agency has released draft risk evaluations for four chemicals: PV-29, HBCD, 1,4-dioxane, and 1-bromopropane. I’ve been working with my former colleagues at EDF Health to carefully review the drafts for the latter two chemicals. Unfortunately, as expected, these drafts put out by the Trump EPA have a number of problems, which we’ve detailed in public comments.
Last week, we published a meta-analysis that found that high exposure to glyphosate-based herbicides was associated with an increased risk of non-Hodgkin Lymphoma (NHL). There was a lot of discussion about this paper in the news, on social media, and across internet forums (as expected, given the ongoing controversy and high stakes of this conclusion). Most articles focused on the specific risk estimate that we reported, with headlines such as:
A common critique of these headlines (and our article) was that they (and we) were being misleading, because we reported the 41% increased relative risk of NHL – which sounds very scary!—rather than a 0.8% increased absolute risk of NHL – which sounds less scary.
At the risk of more undue attention on the 41% number (which as I said in my previous post, is less important than the finding of a significant association itself), let me explain a few things about (1) how we report results in epidemiological research, (2) why small increases in risk matter, and (3) how agencies like the Environmental Protection Agency (EPA) regulate on risk.
Relative risks vs. absolute risks
In epidemiology, we are trying to understand whether an exposure is associated with a disease. To do this, we compare the disease rate in the exposed group with the disease rate in the unexposed group. This ratio gives us the relative risk of disease between the two groups.
[Side note: this is why it is crucial for researchers to select an appropriate comparison group! The relative risk depends entirely on this decision! If your comparison group has an unusually high rate of cancer, you will get a very skewed (and wrong) answer about the effects of the exposure.]
This relative risk, however, does not give us any information on the absolute risk of the disease at the individual level. It only tells us whether the exposed group has a higher or lower chance of developing the disease than the comparison group. In our paper, we report that individuals with high exposure to glyphosate-based herbicides (for example, people who spray it daily for many years) have a 41% increased risk of developing NHL over their lifetimes, compared to those who were not highly exposed (infrequent or no history of use).
The absolute risk, by contrast, tells us the actual risk of the disease for a given level of exposure. This is much more intuitive. For example, on average in the US, approximately 2 out of every 100 people develop NHL during their lifetime. So, the absolute risk of NHL over a lifetime is 2%. Therefore, when our study reports a 41% increased risk for those who are highly exposed, that is equivalent to saying that these individuals now have an absolute risk of 2.8% risk of NHL.
These statistics are communicating the same basic information, but they sound very different. In our epidemiology courses, we learn that absolute risk is better for communicating to the public because it is easier to understand. But, because of the way that epidemiological studies are designed (comparing disease rates in one group vs. the other), our default is to report relative risks. And because we are used to thinking about these ratios, we don’t always realize that this information can be misinterpreted, misunderstood, and confusing. Maybe we should report both metrics in our abstracts.
Nevertheless, both ways of talking about risk give us the same answer to the central question of carcinogenicity: evidence suggests that glyphosate exposure is associated with an increased risk of cancer.
Why seemingly low risks are still important
Some environmental exposures have very high relative risks. Individuals exposed to high levels of asbestos in their homes, for example, have an 800% increased risk of developing mesothelioma, a very rare type of lung cancer.
Most common environmental exposures, however, are associated with relatively small increased relative risks. Let’s take a look at air pollution, a very common exposure. And more specifically, fine particulate matter (PM2.5), very tiny particles emitted from vehicles, industrial facilities, and fires. While exact estimates vary based on the population studied, an increased concentration (of 10 ug/m3, to be exact) in 24-hour average PM2.5 has been associated with a 0.4%-1.0% increased risk of death (mostly from cardiovascular disease). An increase (again, of 10 ug/m3) in long term average PM2.5 has been associated with an overall 10% increased risk of death.
Those seem like small changes in risk. So, can we stop worrying about air pollution?
No, definitely not.
Low relative risks applied to large populations can be extremely consequential. We are all exposed to air pollution. Everyday. And all of those exposures add up. In fact, PM2.5 was ranked as the 5th most important cause of death around the world in 2015, accounting for approximately 4.2 million deaths.
Glyphosate-based herbicides are the most heavily used herbicides in the world, with an estimated 1.8 billion pounds applied in 2014. Most of this usage is on commercial agricultural farms by workers with potentially high cumulative exposures over their lifetimes. Given the large number of people possibly exposed, any significant increase in risk – especially the 41% estimate that we report – is meaningful to consider at the population level.
Regulating risk
Finally, I want to bring up a point about cancer risk in relation to regulations. The US EPA and Food and Drug Administration (FDA), among other agencies, have to manage and regulate risks for the population. For most scenarios, they have decided that an “acceptable risk” for a carcinogen in the general population is between 1 in a million and 1 in 10,000 (over a lifetime). In other words, EPA and FDA are supposed to take action to prevent exposure to carcinogens that would result in risks higher than those rates (the specific threshold depends on the scenario and, sometimes, technologic feasibility).
Our findings suggest that the absolute risk of NHL over a lifetime might shift from approximately 2% to 2.8% with high exposure to glyphosate-based herbicides. This difference represents an increase of 8/1000 – certainly above EPA’s threshold of concern for the general population.
Note, however, that some of the studies in our meta-analysis were focused on people using glyphosate in commercial agricultural settings. EPA usually allows a higher risk of cancer in occupational scenarios, approximately 1 in 1000. Even with that standard, however, our results would suggest a need for action.
I’m just using these comparisons to put our results in context, because many people seemed to discount this work because of the small absolute risk estimates. Before any actual regulatory action, EPA would need to consider extensive evidence on hazard and exposure in a formal risk assessment.
Summary
In closing, I hope that I’ve clarified a few points about risk that were raised in the aftermath of the glyphosate publication. But once again, let me emphasize that you should not focus too much on the specific numerical estimates above but rather use them to better understand that:
Relative risks are different than absolute risks. Epidemiologists usually use relative risks, so that is what you will see in published papers (and, likely, the headlines as well).
Exposures with low relative risks can still have huge impacts at the population level.
Regulatory agencies set certain benchmarks for acceptable lifetime cancer risk in the population. You might not agree with the thresholds, but those are the standards. Keep that in mind when you are reading about risks from environmental exposures.
Apologies for the long blog absence. I’ve been busy PhD-ing (including preparing for and passing my oral general exam!) and working on various side projects.
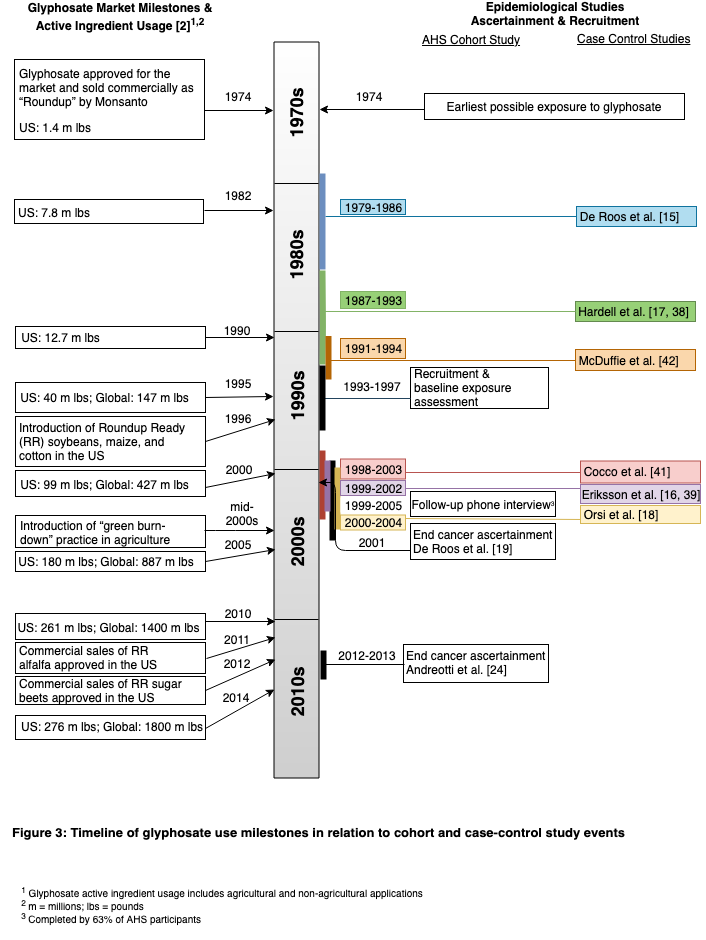
One of those side projects has been focused on glyphosate. Glyphosate, the active ingredient in Monsanto’s (now owned by Bayer) Roundup, is the most widely used herbicide in the world. First marketed in 1974, its usage skyrocketed after the introduction of “Roundup-ready” (i.e.: Roundup resistant) crops in 1996 and the practice of “green-burndown” (i.e.: using the chemical as a desiccant shortly before harvest) in the mid-2000s. In 2014, global usage was estimated to be 1.8 billion pounds.
But these staggering statistics are not the only claim to fame for glyphosate. It has also been the subject of intense international regulatory and scientific scrutiny in recent years, for its possible link to cancer. The stakes are high (billions of dollars for Monsanto, related to sales of both the herbicide itself and its line of herbicide-resistant crops), and the conclusions are controversial.
Carcinogenic or not, that is the question.
In 2015, the International Agency on Cancer (IARC) declared that glyphosate was a “probable human carcinogen” (relevant links: explanation of IARC classifications; official summary for glyphosate; IARC webpage with follow-up links). However, that same year, the European Food Safety Authority (EFSA) concluded that “glyphosate is unlikely to pose a carcinogenic hazard to humans, and the evidence does not support classification with regard to its carcinogenic potential.” In 2016, the US Environmental Protection Agency (EPA) determined that glyphosate was “not likely to be carcinogenic to humans at doses relevant for human health risk assessment.”
Ok, so that’s confusing. How did these agencies, all of which are supposed to conduct unbiased reviews of all of the evidence come to such different conclusions? There have been several recent publications that explain these inconsistencies (for example, see here and here). In essence, it boils down to: 1) differences in how the agencies weighed peer-reviewed, publicly available studies (most show adverse health effects) versus unpublished regulatory studies submitted by manufacturers (most do not show adverse health effects); 2) whether the agencies focused on studies of pure glyphosate or the final formulated glyphosate-based product that is used in agricultural applications (which is known to be more toxic); and 3) whether the agencies considered dietary exposures to the general population only or also took into account elevated exposures in occupational scenarios (i.e. individuals who apply glyphosate-based herbicides in agricultural settings).
Meanwhile, as the debate continues… 27 countries (as of November 2018) have decided to move forward with implementing their own bans or restrictions. And, Monsanto/Bayer faces more than 9,000 lawsuits in the US from individuals who link their cancer to the herbicide. (The courts ruled the first case in favor of the plaintiff, though Monsanto is appealing the decision).
My connection
This highly contentious area is outside the topic of my dissertation research, but I got involved because my advisor was a member of the EPA scientific advisory panel that reviewed the agency’s draft assessment of glyphosate in 2016. The panel’s final report raised a number of concerns with EPA’s process and conclusions, including that the agency did not follow its own cancer guidelines and made some inappropriate statistical decisions in the analysis.
Because of their dissatisfaction with EPA’s report, my advisor and two other panel members decided to pursue related research to dig further into the issues. I enthusiastically accepted the invitation to join.
Our collaborative group recently published two review papers on glyphosate. I’ll provide brief highlights of both below.
Reviewing our reviews, part 1: exposure to glyphosate
In January 2019, we published a review of the evidence of worldwide exposure to glyphosate. Even though glyphosate-based products are the most heavily used herbicides in the world, we were surprised (and dismayed) to find less than twenty published studies documenting exposure in only 3721 individuals.
So, our paper mostly serves to highlight the limitations of the existing data:
These studies sampled small numbers of individuals from certain geographic regions, mostly in the US and Europe, and therefore are not representative of the full scope of global exposures
Most studies relied on a single urine spot sample, which does not represent exposure over the long term and/or in different agricultural seasons
The occupational studies only covered 403 workers in total, a serious deficiency given its widespread agricultural use. Few assessed exposure before and after spraying; and no studies evaluated patterns related to seasonality, crop use, etc.
Only two small studies evaluated how population exposure has changed over time. So, we definitely don’t know enough about whether the dramatic increases in global usage have resulted in similarly dramatic increased concentrations in our bodies. (Presumably, yes).
In addition to highlighting the need to address the points above, we specifically recommended incorporating glyphosate into the National Health and Nutrition Examination Survey (NHANES), a national survey that monitors exposure to many chemicals – including other common pesticides. This is an obvious and fairly straightforward suggestion; in reality, it’s quite bizarre that it has not already been incorporated into NHANES. Testing for glyphosate would allow us to better understand exposure across the US – which is not reflective of global levels, of course, but an important start.
Reviewing our reviews, part 2: glyphosate & non-Hodgkin Lymphoma (NHL)
Our second paper, published earlier this week, was a meta-analysis of the link between glyphosate exposure and non-Hodgkin Lymphoma (NHL). Yes, diving right in to the controversy.
There had already been several prior meta-analyses that showed an association between glyphosate and NHL, but ours incorporates new research and applies a method that would be more sensitive to detecting an association.
A meta-analysis combines results from separate studies to better understand the overall association. While they technically do not generate any “new” data, meta-analyses are essential in the field of public health. A single study may have certain weaknesses, focus only on selected populations, or reflect a chance finding. In drawing conclusions about hazards (especially in this scenario, affecting millions of people and billions of dollars), we want to look across the collection of data from many studies so we can be confident in our assessment.
We were able to include a newly published follow-up study of over 54,000 licensed pesticide applicators (part of the Agricultural Health Study (AHS)). Compared to an earlier paper of the same cohort, this updated AHS study reports on data for an additional 11-12 years. This extension is important to consider, given that cancer develops over a long period of time, and shorter studies may not have followed individuals long enough for the disease to arise.
We conducted this meta-analysis with a specific and somewhat unusual approach. We decided to focus on the highly exposed groups in order to most directly address the question of carcinogenicity. In other words, we would expect the dangers (or, proof of safety: is it safe enough to drink?) to be most obvious in those who are highly exposed. Combining people who have low exposure with those who have high exposure would dilute the association. IMPORTANT NOTE: this approach of picking out the high exposure groups is only appropriate because we are simply looking for the presence or absence of a link. If you were interested in the specific dose-response relationship (i.e.: how a certain level of exposure relates to a certain level of hazard), this would not be ok.
Our results indicate that individuals who are highly exposed to glyphosate have an increased risk of NHL, compared to the control/comparison groups. This finding itself is not entirely earth-shattering: the results from prior meta-analyses were similar. But, it adds more support to the carcinogenic classification.
More specifically, we report a 41% increased risk. For comparison, the average lifetime risk of NHL is about 2%. However, I want to emphasize that because our analytical method prioritized the high exposure groups, the precise numerical estimate is less important than the significant positive correlation. Basically, the purpose of this and other related assessments (like IARC’s) is to understand whether glyphosate is carcinogenic or not: this is a yes/no question. It is up to regulatory agencies to judge the scale of this effect and decide how to act on this information.
As with any scientific project, there are several limitations. In particular, we combined estimates from studies that differed in important ways, including their design (cohort vs. case-control), how they controlled for confounding by exposure to other pesticides, and which reference group they chose for the comparison (unexposed vs. lowest exposed). When studies are very different, we need to be cautious about combining them. This is another reason to focus more on the direction of the effect rather than the exact numerical estimate.
Beyond the headlines
The news coverage of this work has focused on the overarching results (especially the 41% statistic), as expected. But I want to highlight a few other aspects that have been overlooked.
To better understand the timing of these studies in relation to glyphosate usage, we put together a timeline of market milestones and epidemiological study events.
This took me SO MANY HOURS.
Of note is that all of the studies conducted to date evaluated cancers that developed prior to 2012-2013, at the latest. Most were much earlier (80s, 90s, early 00s). As illustrated in the timeline, we’ve seen a huge increase in glyphosate usage since green burndown started in the mid-2000s. Yet none of these studies would have captured the effects of these exposures, which means the correlation should be easier to see in newer studies if/when they are conducted.
Also, as I mentioned above, we included the newly published AHS cohort study in our meta-analysis. One might expect the old and new AHS studies to be directly comparable, given that they were conducted by the same research group. However, our deep dive into both papers elucidated important differences; consequently, they are not directly comparable (see Table 8 of our paper). An in-depth discussion of these issues (and some of their potential implications) is a topic for a separate post, but there’s a clear lesson here about how important it is to carefully understand study design and exposure assessment methods when interpreting results.
Finally, two brief points on the animal toxicology studies, which we also reviewed in our paper because they provide complementary evidence for assessing hazard in humans. We discuss these data but did not conduct a formal pooled analysis (to combine results from separate but similarly designed animal studies), which would allow us to better understand overarching results from the animal studies. Anyone ready for a project?
In future animal toxicology studies, researchers should use the formulated glyphosate product that is actually used around the world rather than the pure glyphosate chemical that has been the focus of prior testing. There is growing evidence to suggest that the final formulated product is more toxic, perhaps due to the added adjuvants and surfactants. And this would allow for better comparisons to the human epidemiological studies, which assess effects of exposure to the formulated product.
Reflecting on the process
I had followed the evolving story on glyphosate with great interest for several years, so it was exciting to be part of these projects. Contributing to research with a real-world public health impact has always been a priority for me, and this high-profile research (affecting millions of people, billions of dollars) certainly fits the bill.
That being said, it was not an easy process. These two papers represent years of work by our group, which we did on top of our regular commitments. Collaborating with three researchers whom I had never met also proved challenging, since we did not have established rapport or an understanding of each other’s work and communication styles. So, in addition to gaining skills in conducting literature reviews and meta-analyses, I learned valuable lessons in group dynamics. 🙂
Given the high-stakes and high-profile nature of this work, we were extra meticulous about the details of this project. We knew that it would be scrutinized carefully, and any error could damage our credibility (especially worrisome for me, since I’m just establishing myself in my career). It took many, many rounds of review and editing to get everything right. A good lesson in patience.
Speaking of patience, I know that scientific research and related policy decisions take time. But I hope that these two projects can contribute to moving forward in a direction that protects public health.
In recent years, national and international environmental public health organizations (including the US Environmental Protection Agency and the World Health Organization) have begun to use the adverse outcome pathway (AOP) and/or mode of action (MOA) as unifying frameworks for chemical testing and risk assessment. While the details of these frameworks vary, their underlying ideas are similar: researchers link specific molecular changes caused by environmental chemicals with adverse outcomes at the organism level (ie: disease), and then risk assessment is conducted based on the premise that preventing the early molecular disruption will prevent the development of the end-stage adverse event.
While there are practical advantages and real logic to this mechanism-based approach, a new review article published in Carcinogenesis suggests that this strategy may be overly simplistic and could potentially hinder our ability to adequately identify chemicals that contribute to the development of cancer.
This international team of cancer biologists and environmental health scientists organized their discussion around the “Hallmarks of Cancer,” a list of acquired characteristics that commonly occur in cancer (for example: continued growth, resistance to cell death, and tissue invasion). For each key characteristic, they identified typical target sites for disruption as well as environmental chemicals that have been shown to act on those targets. The researchers focused their discussion solely on chemicals that were not already categorized as human carcinogens by the International Agency for Research on Cancer (IARC), and they took careful note of effects observed at low doses. In addition, they specifically mapped connections between different pathways to highlight cases in which alterations leading to a given cancer hallmark could also lead to another.
Their lengthy review provides an important overview of the procarcinogenic effects of numerous common chemicals, but perhaps the most significant conclusion of this work is to emphasize the pitfalls in the status quo for risk assessment. By focusing on categorizing single chemicals as ‘carcinogens,’ we neglect to acknowledge that combinations of chemicals that individually do not meet criteria to be categorized as ‘carcinogenic’ may act in synergistic ways to promote the development of cancer. Even recent efforts to evaluate the effects of chemical mixtures may be inadequate, as they mostly focus on chemicals with common cellular pathways or targets. What about the numerous compounds, as identified in this review, that act on disparate pathways and organs to contribute to a similar disease process in the body?
To address these problems, the authors propose several key principles for an improved framework for cumulative risk assessment, including consideration of the synergistic activity of:
chemicals that act via different pathways
chemicals that act on different target tissues
non-carcinogens that act at low doses to contribute to pro-carcinogenic processes
chemicals that are not structurally similar
Carcinogenesis, like many disease processes, is complicated, and identifying the numerous pathways and organs involved is – and will continue to be – an enormous scientific challenge. Slow progress can be made, nevertheless, with a shift towards testing real-world combinations of chemicals and by using the ‘Hallmarks of Cancer’ to guide relevant and appropriate research. New technologies, such as high throughput screening, computational modeling and systems biology-based analysis, can aid in this process. However, the authors stress that traditional in vivo testing still holds an important place in cancer-related research – at least until there is appropriate validation of these emerging tools.
This publication highlights that our current chemical testing and risk assessment system is overly narrow and negates the complexity with which chemicals can interact in the body. We must broaden our approach to acknowledge that distinct chemicals can act in distinct ways at distinct sites – even at low doses – to contribute synergistically to a specific disease process. Reframing our perspective is daunting, and it will emphasize our limited knowledge about the mixtures of chemicals that we are exposed to everyday. But, if we can look up to see the forest, we may begin to make our way towards safer territory.